










Gastro-oesophageal Tumor
Access expert guidance on Gastro-oesophageal Tumors, including treatment innovations and dietary management tips, to support patients through their treatment.

The type and grade of cancer are usually clear when the cells are seen under a microscope after routine processing and staining, but this is not always the case. Sometimes the pathologist needs to use other procedures to make a diagnosis.
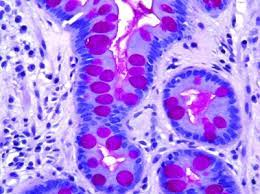
These tests employ a variety of chemical dyes that are drawn to certain chemicals found in cancer cells. The mucicarmine stain, for example, is drawn to mucus. Under a microscope, droplets of mucus inside a cell exposed to this dye will appear pink-red. If a pathologist suspects an adenocarcinoma (a glandular kind of cancer) in a lung sample, this stain can help. Because adenocarcinomas can create mucus, detecting pink-red patches in lung cancer cells will indicate that the diagnosis is adenocarcinoma to the pathologist.
Other sorts of specific stains are employed in the lab to identify microorganisms (germs) like bacteria and fungi in tissues, in addition to sorting out different types of tumors. This is critical because cancer patients may get infections as a result of their treatment or as a result of the disease itself. It's also crucial in cancer diagnosis since some infectious disorders create lumps that can be mistaken for cancer until histochemical stains show that the patient is suffering from an infection rather than cancer.
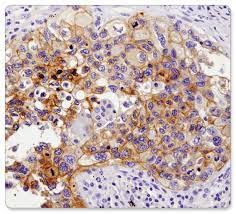
Immunohistochemical (IHC) or immunoperoxidase stains are another class of specific tests that can be highly valuable. The underlying idea behind this strategy is that an immune protein called an antibody will bind itself to particular molecules on or in the cell called antigens. Antibodies identify and adhere to antigens that are specific to them. Normal cells and malignant cells each have their own antigens. If a cell has a specific antigen, the antibody that matches the antigen will be drawn to it. To see if antibodies have been drawn to the cells, chemicals are given that cause the cells to change color only when a certain antibody (and thus the antigen) is present.
Our bodies normally make antibodies that recognize antigens on germs and help protect us against infections. The antibodies used in IHC stains are different. Theyre made in the lab to recognize antigens that are linked to cancer and other diseases.
IHC stains are quite helpful in diagnosing specific malignancies. A routinely processed biopsy of a lymph node, for example, may have cells that clearly appear like cancer, but the pathologist may not be able to tell whether cancer started in the lymph node or spread to the lymph nodes from elsewhere in the body. Lymphoma would be the diagnosis if cancer began in a lymph node. It could be metastatic cancer if cancer started in another place of the body and spread to the lymph node. This difference is critical since treatment options vary depending on the type of cancer (as well as some other factors, too).
There are hundreds of antibodies used for IHC tests. Some are quite specific, meaning that they react only with one type of cancer. Others may react with a few types of cancer, so several antibodies may be tested to decide what type of cancer it is. By looking at these results along with cancers appearance after the biopsy specimen is processed, its location, and other information about the patient (age, gender, etc.), its often possible to classify cancer in a way that can help select the best treatment.
IHC stains are most commonly used to classify cells, however, they can also be used to detect or identify cancer cells. While a substantial number of cancer cells have moved to a nearby lymph node, the pathologist can easily identify these cells using conventional stains when looking at the lymph tissue under the microscope. However, if the node only contains a few cancer cells, it can be difficult to distinguish the cells using simply normal stains. IHC stains can aid in this situation. Once the pathologist has determined the type of malignancy to be examined, he or she might select one or more antibodies that have been shown to react with those cells. More chemicals are added so that the cancer cells will change color and clearly stand out from the normal cells around them. IHC stains are generally not used to look at tissue from lymph node dissections (which remove a large number of nodes), but they are sometimes used in sentinel lymph node biopsies.
Another specialized use of these stains is to help distinguish lymph nodes that contain lymphoma from those that are swollen from increased numbers of normal white blood cells (usually as a response to infection). Certain antigens are present on the surface of white blood cells called lymphocytes. Benign (non-cancerous) lymph node tissue contains many different types of lymphocytes with a variety of antigens on their surface. In contrast, cancers like lymphoma start with a single abnormal cell, so the cancer cells that grow from that cell typically share the chemical features of the first abnormal cell. This is especially useful in diagnosing lymphoma. If most of the cells in a lymph node biopsy have the same antigens on their surface, this result supports a diagnosis of lymphoma.
Some IHC stains can help recognize specific substances in cancer cells that influence a patients prognosis and/or whether they are likely to benefit from certain drugs. For example, IHC is routinely used to check for estrogen receptors on breast cancer cells. Patients whose cells have these receptors are likely to benefit from hormone therapy drugs, which block the production or effects of estrogens. IHC can also help determine which women with breast cancer are likely to benefit from drugs that block the growth-promoting effects of abnormally high levels of the HER2 protein.
The typical medical lab microscope uses a beam of ordinary light to look at specimens. A larger, much more complex instrument called an electron microscope uses beams of electrons. The electron microscopes magnifying power is about 1,000 times greater than that of an ordinary light microscope. This degree of magnification is rarely needed in deciding whether a cell is cancer. But it sometimes helps find very tiny details of a cancer cells structure that provide clues to the exact type of cancer.
Under a standard light microscope, certain cases of melanoma, a highly deadly skin cancer, may appear to be other cancers. The majority of the time, IHC stains can identify these melanomas. If such tests don't reveal anything, an electron microscope can be used to look for microscopic structures called melanosomes inside melanoma cells. This aids in determining the type of cancer and determining the best treatment option.

Flow cytometry is often used to test the cells from bone marrow, lymph nodes, and blood samples. Its very accurate in finding out the exact type of leukemia or lymphoma a person has. It also helps tell lymphomas from non-cancer diseases in the lymph nodes.
A sample of cells from a biopsy, cytology specimen, or blood specimen is treated with special antibodies. Each antibody sticks only to certain types of cells that have the antigens that fit with it. The cells are then passed in front of a laser beam. If the cells now have those antibodies, the laser will make them give off light thats then measured and analyzed by a computer.
Analyzing cases of suspected leukemia or lymphoma by flow cytometry uses the same principles explained in the section on immunohistochemistry:
Flow cytometry can also be used to measure the amount of DNA in cancer cells (called ploidy). Instead of using antibodies to detect protein antigens, cells can be treated with special dyes that react with DNA.
Another use of flow cytometry is to measure the S-phase fraction, which is the percentage of cells in a sample that are in a certain stage of cell division called the synthesis or S phase. The more cells that are in the S-phase, the faster the tissue is growing and the more aggressive the cancer is likely to be.
Like flow cytometry, this test uses dyes that react with DNA. But instead of suspending the cells in a stream of liquid and analyzing them with a laser, image cytometry uses a digital camera and a computer to measure the amount of DNA in cells on a microscope slide. Like flow cytometry, image cytometry also can determine the ploidy of cancer cells.
Normal human cells have 46 chromosomes (pieces of DNA and protein that control cell growth and function). Some types of cancer have one or more abnormal chromosomes. Recognizing abnormal chromosomes helps to identify those types of cancer. This is especially useful in diagnosing some lymphomas, leukemias, and sarcomas. Even when the type of cancer is known, cytogenetic tests may help predict the patients outlook. Sometimes the tests can even help predict which chemotherapy drugs the cancer is likely to respond to.
Several types of chromosome changes can be found in cancer cells:
Sometimes, an entire chromosome might be gained or lost in the cancer cells.
For cytogenetic testing, cancer cells are grown in lab dishes for about 2 weeks before their chromosomes can be looked at under the microscope. Because of this, it usually takes about 3 weeks to get results.
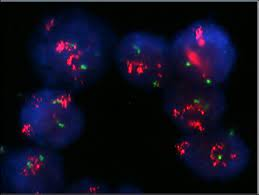
FISH, or fluorescent in situ hybridization, is similar to cytogenetic testing. It can detect the majority of chromosomal alterations visible under a microscope in routine cytogenetic tests. It can also detect changes that are too tiny to be detected by traditional cytogenetic testing.
FISH makes use of fluorescent dyes that are linked to DNA fragments that only connect to specific sections of chromosomes. FISH can detect chromosome alterations such as translocations, which are useful in classifying certain types of leukemia.
Finding certain chromosome changes is also important in determining if certain targeted drugs might help patients with some types of cancer. For example, FISH can show when there are too many copies (called amplification) of the HER2 gene, which can help doctors choose the best treatment for some women with breast cancer.
Unlike standard cytogenetic tests, its not necessary to grow cells in lab dishes for FISH. This means FISH results are available much sooner, usually within a few days.
Other tests of DNA and RNA can be used to find most of the translocations found by cytogenetic tests. They can also find some translocations involving parts of chromosomes too small to be seen under a microscope with usual cytogenetic testing. This type of advanced testing can help classify some leukemias and, less often, some sarcomas and carcinomas. These tests are also useful after treatment to find small numbers of remaining leukemia cancer cells that may be missed under a microscope.
Molecular genetic tests can also identify mutations (abnormal changes) in certain areas of DNA that control cell growth. Some of these mutations may make cancers especially likely to grow and spread. In some cases, identifying certain mutations can help doctors choose treatments that are more likely to work.
Certain substances called antigen receptors are on the surface of immune system cells called lymphocytes. Normal lymph node tissue contains lymphocytes with many different antigen receptors, which help the body respond to infection. But some types of lymphoma and leukemia start from a single abnormal lymphocyte. This means all these cancer cells have the same antigen receptor. Lab tests of the DNA of each cells antigen receptor genes are a very sensitive way to diagnose and classify these cancers.
Polymerase chain reaction (PCR): This is a very sensitive molecular genetic test for finding specific DNA sequences, such as those occurring in some cancers. Reverse transcriptase PCR (or RT-PCR) is a method used to detect very small amounts of RNA. RNA is a substance related to DNA thats needed for cells to make proteins. There are specific RNAs for each protein in our body. RT-PCR can be used to find and classify cancer cells.
An advantage of RT-PCR is that it can detect very small numbers of cancer cells in blood or tissue samples that would be missed by other tests. RT-PCR is used routinely for detecting certain kinds of leukemia cells that remain after treatment, but its value for more common types of cancer is less certain. The disadvantage is that doctors are not always sure whether having a few cancer cells in the bloodstream or a lymph node means that a patient will actually develop distant metastases that will grow enough to cause symptoms or affect survival. In treating patients with the most common cancer types, its still not clear whether finding a few cancer cells with this test should be a factor in choosing treatment options.
RT-PCR can also be used to sub-classify cancer cells. Some RT-PCR tests measure levels of one or even several RNAs at the same time. By comparing the levels of important RNAs, doctors can sometimes predict whether a cancer is likely to be more or less aggressive (likely to grow and spread) than would be expected based on how it looks under the microscope. Sometimes these tests can help predict whether cancer will respond to certain treatments.
Gene expression microarrays: These tiny devices are in some ways like computer chips. The advantage of this technology is that relative levels of hundreds or even thousands of different RNAs from one sample can be compared at the same time. The results tell which genes are active in a tumor. This information can sometimes help predict a patients prognosis (outlook) or response to certain treatments.
This test is sometimes used when cancer has spread to several parts of the body but doctors arent sure where it started. (These are called cancers of unknown primary.) The RNA pattern of these cancers can be compared with the patterns of known types of cancer to see if they match. Knowing where cancer started is helpful in choosing treatment. These tests can help narrow down the cancer type, but they are not always able to tell the exact type of cancer with certainty.
DNA sequencing: For the past couple of decades, DNA sequencing has been used to identify people who have inherited genetic mutations that greatly increase their risk of developing certain types of cancer. In this case, the testing generally uses DNA from blood cells of either patients who already have certain cancers (such as breast cancer or colon cancer) or from the blood of their relatives who do not have any known cancer but may be at increased risk.
Doctors have started using DNA sequencing of some cancers to help predict which targeted drugs are most likely to work in individual patients. This practice is sometimes called personalized oncology or precision oncology. At first, DNA sequencing was done for only one gene or for a few genes that were known to be most often affected for certain types of cancer. Recent progress has made it possible to sequence many more genes or even all of the genes from cancer (although this is still not done routinely). This sequence information sometimes shows unexpected mutations in genes that are affected less often and may help the doctor choose a drug that otherwise would not have been considered and avoid other drugs that are unlikely to be helpful.
 Link Copied
Link Copied




Nurture Hope & Healing
with ZenOnco
On Google play India



Nurture Hope & Healing
with ZenOnco
On Google play India



